- Home
- About Us
- Contact Us
- Biography
- Column
- MedBound Hub
- InternshipInternship
- Daily Pulse
- Medicine
- Physical Therapy
- InterviewInterview
- Pharmacy
- Biotechnology
- College/InstituteCollege/Institute
- Dentistry
- Blog
- Wellness & Nutrition
- Nursing
- Opinion

With growing digitalization and increasing dependence on gadgets such as computers, smartphones, and gaming devices, posture-related problems have become increasingly common. Long hours spent working on laptops, desktop computers, or gaming consoles often lead to symptoms such as wrist discomfort, numbness, tingling, or weakness in the hand.
At the same time, wrist braces have become increasingly popular among office workers, students, programmers, gamers, and remote workers. However, many individuals begin using these devices without fully understanding the anatomical principles behind their design and function.
One of the primary purposes of wrist braces is to maintain neutral wrist alignment and reduce mechanical stress on structures within the wrist, particularly the median nerve.
Compression of this nerve within the carpal tunnel is associated with carpal tunnel syndrome, one of the most common nerve compression disorders affecting the upper limb.
Understanding the anatomy of the median nerve and the carpal tunnel can help explain why wrist position plays such an important role in wrist health and why wrist braces are designed the way they are.
The median nerve is one of the major nerves of the upper limb and is responsible for many of the hand movements and sensations we rely on every day.1 Activities such as typing, writing, gripping objects, and using a smartphone depend on the proper functioning of this nerve.
The median nerve originates from the brachial plexus, a network of nerves formed by spinal nerve roots C5 to T1. It travels from the neck through the arm and forearm before entering the hand, giving off branches that supply several muscles along its course.
The median nerve provides motor supply to most of the flexor muscles of the forearm and several muscles in the hand that control thumb movement and fine motor skills. It is particularly important for thumb opposition, a movement essential for gripping and handling objects.
It also carries sensory information from the thumb, index finger, middle finger, and the lateral half of the ring finger, as well as part of the palm.
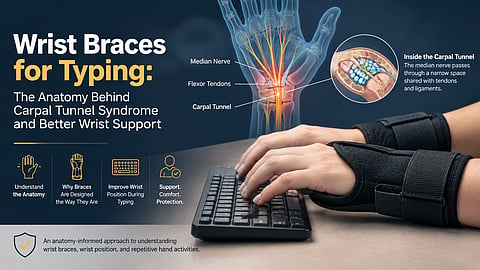
At the wrist, the median nerve passes through the carpal tunnel, a narrow space shared with several flexor tendons. Because this tunnel has limited room, swelling of the surrounding tissues or repetitive hand movements can increase pressure within the tunnel and compress the nerve.
This compression can lead to symptoms such as pain, numbness, tingling, and weakness in the hand, characteristic of carpal tunnel syndrome.1
Common manifestations of median nerve compression include:
Tingling or numbness involving the thumb, index finger, middle finger, and radial half of the ring finger.
Symptoms that worsen at night.
Weakness while gripping objects.
Difficulty performing thumb opposition.
Thenar muscle wasting in advanced cases.² ⁴
This placement is ideal because you're already discussing compression and symptoms.
Carpal tunnel syndrome (CTS) is the most common nerve compression disorder worldwide and is a frequent cause of hand pain, numbness, and tingling. 2
To understand why the median nerve becomes compressed, it is important to first understand the anatomy of the carpal tunnel.
The carpal tunnel is a narrow passage located on the palmar side of the wrist. Its floor and side walls are formed by the carpal bones, which are arranged in an arch-like configuration. These bones create a rigid framework that provides protection and support for the structures passing through the tunnel.
The roof of the carpal tunnel is formed by a strong fibrous band known as the transverse carpal ligament also known as the flexor retinaculum. This ligament stretches across the carpal arch, converting it into a tunnel and helping to keep the flexor tendons in place during hand and finger movements.
The carpal tunnel contains the median nerve along with nine flexor tendons responsible for finger and thumb movements. These structures pass through the tunnel as they travel from the forearm into the hand.
Unlike other soft tissue compartments, the carpal tunnel has very little capacity to expand because it is bounded by bones on three sides and a strong ligament on the fourth. As a result, even minor swelling of the tendons or surrounding tissues can increase pressure within the tunnel and compress the median nerve, leading to the symptoms associated with carpal tunnel syndrome.3,4
See also: Do You Always Keep Your Phone in Your Pocket? It May Lead to Sore Thighs
Most people think typing is a low-effort activity, but the hands and wrists are constantly at work. Whether you are typing emails, writing reports, coding, or gaming, your fingers perform thousands of small movements throughout the day. Over time, this repetitive activity can place stress on the structures that pass through the wrist.
Every time you press a key, tendons in your fingers and forearm slide back and forth to create movement. While these motions are natural, hours of continuous typing with few breaks, repetitive hand movements or keeping the wrist in awkward positions for long periods may increase stress on the structures inside the wrist and can worsen symptoms for some people. Carpal tunnel syndrome has many causes, and factors such as obesity, diabetes, hypothyroidism, pregnancy, rheumatoid arthritis, and inherited traits can also increase the risk.
The position of the wrist is just as important as the amount of typing. A neutral wrist position, where the hand remains aligned with the forearm, places the least amount of stress on the structures within the carpal tunnel. However, when the wrist is held in a bent position, either upward (extension) or downward (flexion), the space available inside the tunnel can become more restricted.
The wrist does not work in isolation. Poor desk setup, prolonged mouse use, and maintaining the same position for extended periods can all affect the way forces are distributed across the wrist. Even small changes in wrist angle can increase pressure on the tendons and median nerve. This helps explain why posture and ergonomics are often emphasized when discussing wrist discomfort associated with computer use.5
At first glance, a wrist brace may seem like a simple support device. However, its design is based on the anatomy and biomechanics of the wrist. The goal is not to immobilize the hand completely, but to keep the wrist in a position that places the least amount of stress on the structures within the carpal tunnel.
Although wrist braces may help maintain wrist alignment and are commonly used in conservative management of mild-to-moderate carpal tunnel syndrome, they do not address every cause of wrist pain and are not a substitute for medical evaluation when symptoms persist. Evidence supporting their use for preventing carpal tunnel syndrome in healthy individuals is limited.⁶⁻⁸
One of the main functions of a wrist brace is to support the wrist in a neutral position, where the hand remains aligned with the forearm. This position is generally associated with less pressure on the median nerve and the tendons passing through the carpal tunnel.
Many daily activities involve bending the wrist forward or backward without us even realizing it. Wrist braces are designed to limit these extreme movements because prolonged flexion or extension can reduce the available space within the carpal tunnel and increase stress on its contents.
If you have ever noticed a metal or plastic strip inside a wrist brace, that is the splint. Its purpose is to help the wrist maintain a stable position, especially during sleep when wrist posture is difficult to control. By preventing excessive movement, the splint helps reduce unnecessary mechanical stress on the wrist.
Many individuals with carpal tunnel syndrome experience nocturnal symptoms because the wrist may unintentionally flex during sleep, increasing pressure within the carpal tunnel. This is one reason symptoms often become more noticeable at night and why night splints are commonly recommended as part of conservative treatment.² ⁶
The design of a wrist brace closely follows the anatomy of the wrist. Its shape supports the natural alignment of the joint while allowing the fingers to move freely. Features such as adjustable straps, built-in splints, and targeted support are intended to stabilize the wrist without interfering with everyday hand function.6,7
Choosing a wrist brace is not simply about picking the most rigid or heavily padded option. Since wrist braces are designed to work with the natural anatomy of the wrist, their effectiveness often depends on how well they support proper alignment while remaining comfortable to wear.
A good wrist brace should help keep the wrist in a neutral position, where the hand is aligned with the forearm. This position places the least amount of stress on the median nerve and the tendons that pass through the carpal tunnel. Because of this, neutral wrist alignment is one of the key principles behind the design of most wrist braces.
The fit of a wrist brace is just as important as its design. A brace that is too loose may not provide adequate support, while one that is too tight can become uncomfortable and place unnecessary pressure on the surrounding tissues. Since wrist size and shape vary from person to person, selecting a properly fitting brace helps ensure both comfort and effective support.
Not all wrist braces serve the same purpose. Nighttime braces are often designed to provide greater stability because many people unknowingly bend their wrists while sleeping. Daytime braces, in contrast, tend to be lighter and less restrictive, allowing everyday activities to be performed while still offering support to the wrist.
More support does not always mean better support. While a brace should limit positions that place excessive stress on the wrist, it should also allow enough movement for normal hand function. For this reason, many wrist braces combine supportive splints with flexible materials, creating a balance between stability and comfort.8
Night splints are recommended as a conservative treatment option for many patients with mild-to-moderate carpal tunnel syndrome. Wrist braces may help relieve symptoms by maintaining the wrist close to its natural alignment and reducing pressure within the carpal tunnel. However, they do not cure severe disease. Persistent numbness, weakness, worsening symptoms, or visible thinning of the muscles at the base of the thumb should not be ignored and warrant medical evaluation. In advanced cases, surgery may be needed to relieve pressure on the median nerve.
Keep the wrists close to neutral during typing and repetitive activities.
Take short breaks every 30 to 60 minutes.
Night splints may help relieve mild carpal tunnel syndrome symptoms.
Wrist braces are supportive devices and not cures.
Persistent numbness, weakness, or loss of hand function warrants medical evaluation.
Most of us spend hours every day typing, scrolling, clicking, or gaming without giving much thought to what is happening inside our wrists. Yet, a small structure like the median nerve passes through a very confined space called the carpal tunnel, where even minor changes in wrist position can affect the surrounding tissues.
This is why wrist braces are designed the way they are. They are not just accessories or supportive bands worn around the wrist. Their design is based on the anatomy of the wrist and aims to keep the joint in a position that places the least amount of stress on the median nerve and the tendons passing through the carpal tunnel.
Understanding the relationship between the median nerve, carpal tunnel, tendons, and ligaments helps explain why posture and wrist positioning matter during typing and other repetitive hand activities. The next time you see a wrist brace, you will know that its design is rooted in anatomy, not just comfort.
1. Kenhub. “The Median Nerve.” Accessed June 19, 2026. https://www.kenhub.com/en/library/anatomy/the-median-nerve.
2. Dahlin, Lars B., Malin Zimmerman, Maurizio Calcagni, Caroline A. Hundepool, Nens van Alfen, and Kevin C. Chung. “Carpal Tunnel Syndrome.” Nature Reviews Disease Primers 10, no. 1 (2024): 37. https://doi.org/10.1038/s41572-024-00521-1.
3. Joshi, Amit, Karan Patel, Ahmed Mohamed, Shrey Oak, Michael H. Zhang, Howard Hsiung, Andy Zhang, and Ujal K. Patel. “Carpal Tunnel Syndrome: Pathophysiology and Comprehensive Guidelines for Clinical Evaluation and Treatment.” Cureus 14, no. 7 (2022): e27053. https://doi.org/10.7759/cureus.27053.
4. Padua, Luigi, Chiara Cuccagna, Stefano Giovannini, and colleagues. “Carpal Tunnel Syndrome: Updated Evidence and New Questions.” The Lancet Neurology 22, no. 3 (2023): 255–267. https://doi.org/10.1016/S1474-4422(22)00432-X.
5. Shiel, William C. “Wrist Pain from Keyboard and Mouse Use: Tendonitis, Nerve Compression, or Joint Instability?” ePainAssist. Accessed June 19, 2026. https://www.epainassist.com/joint-pain/wrist-pain/wrist-pain-from-keyboard-and-mouse-use-tendonitis-nerve-compression-or-joint-instability.
6. Figueiredo, Danielle Soares, Rafaela Rocha Ariboni, Helga Tatiana Tucci, and Raquel de Paula Carvalho. “Effects of Wrist Orthoses in Reducing Pain in Individuals with Carpal Tunnel Syndrome: A Systematic Review.” Disability and Rehabilitation 46, no. 23 (2024): 5395–5403. https://doi.org/10.1080/09638288.2023.2301019.
7. Georgiew, Filip Serż, Jakub Florek, Sebastian Janowiec, and Paweł Florek. “The Use of Orthoses in the Treatment of Carpal Tunnel Syndrome: A Review of the Literature from the Last 10 Years.” Reumatologia 60, no. 6 (2022): 408–412. https://doi.org/10.5114/reum.2022.123681.
8. American Academy of Orthopaedic Surgeons. Management of Carpal Tunnel Syndrome Evidence-Based Clinical Practice Guideline. Rosemont, IL: American Academy of Orthopaedic Surgeons, 2024. https://www.aaos.org/quality/quality-programs/upper-extremity-programs/carpal-tunnel-syndrome/
9. Figueiredo, Danielle Soares, Rafaela Rocha Ariboni, Helga Tatiana Tucci, and Raquel de Paula Carvalho. “Effects of Wrist Orthoses in Reducing Pain in Individuals with Carpal Tunnel Syndrome: A Systematic Review.” Disability and Rehabilitation 46, no. 23 (2024): 5395-5403. https://doi.org/10.1080/09638288.2023.2301019.
10. Georgiew, Filip Serż, Jakub Florek, Sebastian Janowiec, and Paweł Florek. “The Use of Orthoses in the Treatment of Carpal Tunnel Syndrome: A Review of the Literature from the Last 10 Years.” Reumatologia 60, no. 6 (2022): 408-412. https://doi.org/10.5114/reum.2022.123681.
11. Padua, Luigi, Chiara Cuccagna, Stefano Giovannini, et al. “Carpal Tunnel Syndrome: Updated Evidence and New Questions.” The Lancet Neurology 22, no. 3 (2023): 255-267. https://doi.org/10.1016/S1474-4422(22)00432-X.